“Has global health been subverted?” was a question originally posed by Cash and Patel (The Lancet, May 2020) during the early stage of the pandemic. “For the first time in the post-war history of epidemics, there is a reversal of which countries are most heavily affected by a disease pandemic,” they claimed. Official mortality data supported the statement, as did the fact that the pandemic was still in its beginning. But the idea persisted and the official mortality data continued to inspire, up through the present day, the impression that COVID-19 is a rich-country disease.
However, official data have fooled us more than once during this pandemic. The impression that the pandemic has left developing countries unscathed or that COVID-19 has been mild for them could not be further from the truth. This post will show that developing countries were dealt the heaviest blows. So the traditional pattern of which countries are affected the most has not been reversed and global health has not been subverted. This is now – and in fact has always been – mainly a developing country pandemic.
Early on in the pandemic, official mortality data underpinned the claim that COVID-19 would leave the developing world “unscathed”. Later on, again underpinned by official data, this became: the pandemic has been “mild” in developing countries with young populations and therefore they “do not need vaccines”. But none of these claims hold up to scrutiny once we take a broader look.
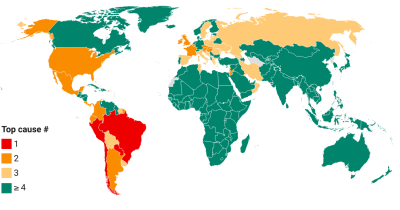
To start the discussion, let us briefly review what the official data tell us. But first a remark on terminology. In what follows, we will be frequently referring to the World Bank income classification of countries. This provides a neat way to divide the world into countries according to their proximate level of development. The classification consists of the groups of high, upper-middle, lower-middle and low income countries. Their respective acronyms are HICs, UMICs, LMICs, and LICs and we will be using these short forms throughout this post.
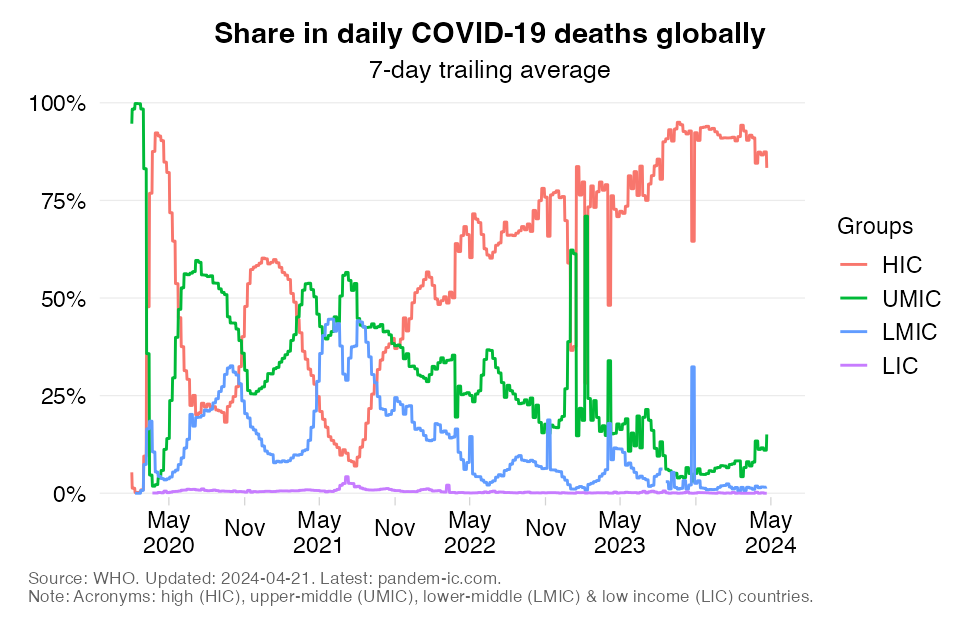
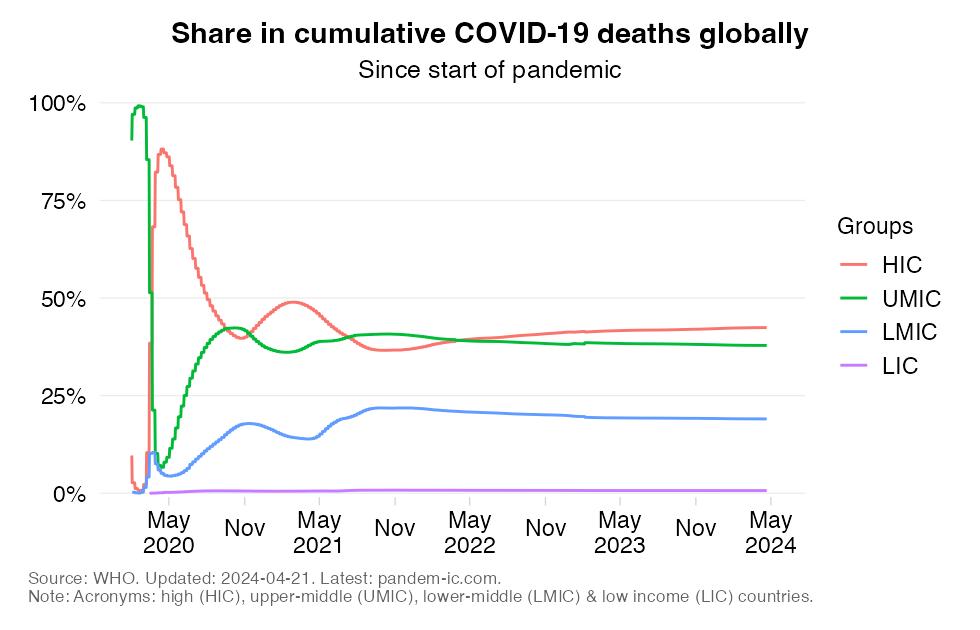
The first thing to note is that the HICs dominate when it comes to the officially published data on COVID-19 mortality. Despite considerable fluctuation, the HIC share in reported COVID-19 mortality remained persistently high as the pandemic matured. In fact, the daily shares reached another peak of 60% around January 2021 and have recently exceeded again the 75% mark (even though of course the global number of deaths is a lot lower now thanks to vaccines). In cumulative terms, we can see that the HIC share seems to have stabilized at around 42%. Even that remains remarkably high, because HICs represent only 15% of the global population.
The high numbers for HICs correlate well with simplistic views about demography. Richer countries have older societies. Moreover, the elderly are more likely to be grouped in care homes. COVID-19 is an age-discriminating disease that penalizes the elderly when infected. Put one, two and three together and the conclusion emerges: COVID-19 is a rich-country disease.
The corollary is that the pandemic would leave the developing countries with their much younger populations “unscathed”. When this turned out to be contradicted even by the official data, this became: the impact on developing countries is “mild” and strongly diluted by the sheer size of the unaffected population. It all seemed to made sense. After all, who would want to contradict official data lending credibility to this view?
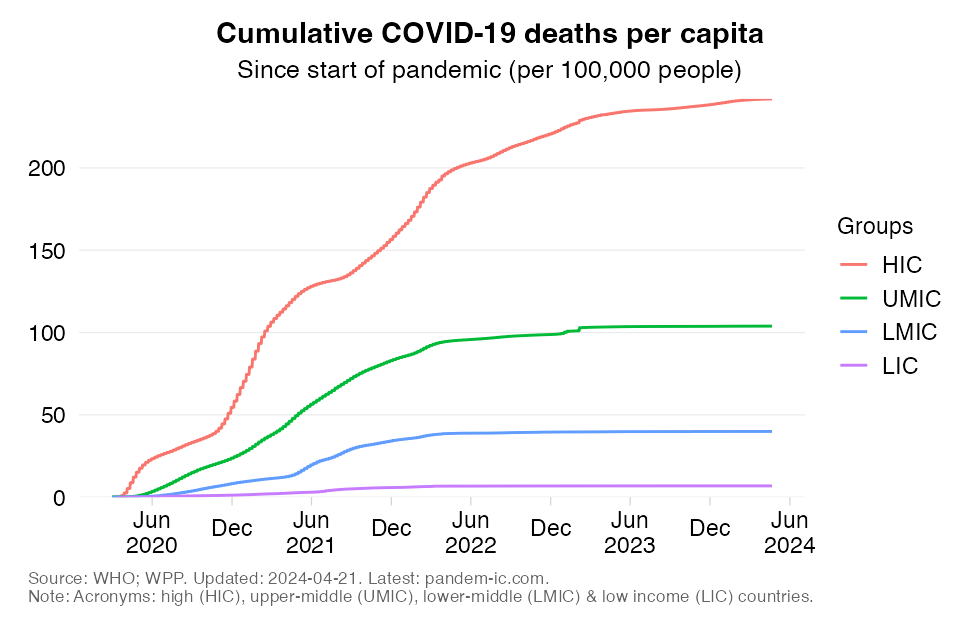
But it didn’t stop here. The argument of a mild developing country pandemic morphed into efforts to undermine the call for global vaccine equity. If HICs suffered the highest mortality rates (as the chart above based on the official data confirms), then why would we need to prioritize other country groups? Even starker, why is there such pressing need to redeploy scarce resources to the LMICs and LICs, which represent the poorer half of the global population, given that their cumulative mortality rates were just a tiny fraction of those of HICs ? And even if vaccines were more abundant, as they are now, why should COVID-19 vaccination deserve priority relative to other pressing health needs in such countries?
The above arguments have two things in common: they are based on poor data and narrow thinking.
Poor data because data quality concerns have been pervasive during the pandemic. Such concerns have been not just the preserve of the developing world – many of the richest HICs have faced difficulties in correctly measuring and attributing COVID-19 as a cause of death. At the same time, we need to recognize that pre-existing inadequacies in CRVS (civil registration and vital statistics) systems before the pandemic will have amplified the challenge of capturing pandemic-related mortality correctly.
Narrow thinking because the mortality toll of the pandemic goes well beyond direct COVID-19 mortality and includes the fatalities that are indirectly related as well as the fatalities that may have been avoided. Examples of additional fatalities include deaths due to unmanaged or undermanaged diseases as resources got redirected to COVID and existing patients became more hesitant to visit hospitals. Examples of deaths that have been avoided include the reduction of other infectious diseases like the flu thanks to mask-wearing and distancing and the avoidance of traffic accidents during lock-downs.
The concept of excess mortality provides a way to redress both of these problems. Excess mortality can be defined as the gap between the total number of deaths that occur for any reason and the number of deaths that would be expected under normal circumstances. To the extent that deaths are captured as part of all-cause mortality, excess mortality estimates pick up a rise in misattributed fatalities. It also captures the broader effects on mortality that are beyond ordinary given previous patterns. In other words, excess mortality addresses the issue of poor data and narrow thinking simultaneously.
Unfortunately, data on all-cause excess mortality are sparsely available, with less than half of all countries providing regular, timely and comprehensive information. This is why exercises to capture the true death toll of the pandemic need to rely on estimates, where excess deaths tend to be estimated directly rather than derived from the difference in observed all-cause mortality and an extrapolated trend. The excess deaths model of The Economist is one such example. It constitutes a colossal attempt to fill the data gaps with estimates based on the information that IS available: over 100 indicators that associate with and help predict excess deaths.
In what follows, we compare the officially reported COVID-19 mortality data and the estimated all-cause mortality data from The Economist. We will take the mid-point estimates. We will differentiate between absolute numbers and relative ones (the mortality rates). Finally, we will make the comparisons by World Bank income classification, World Bank region and UN subregion.
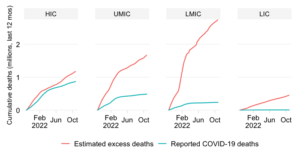
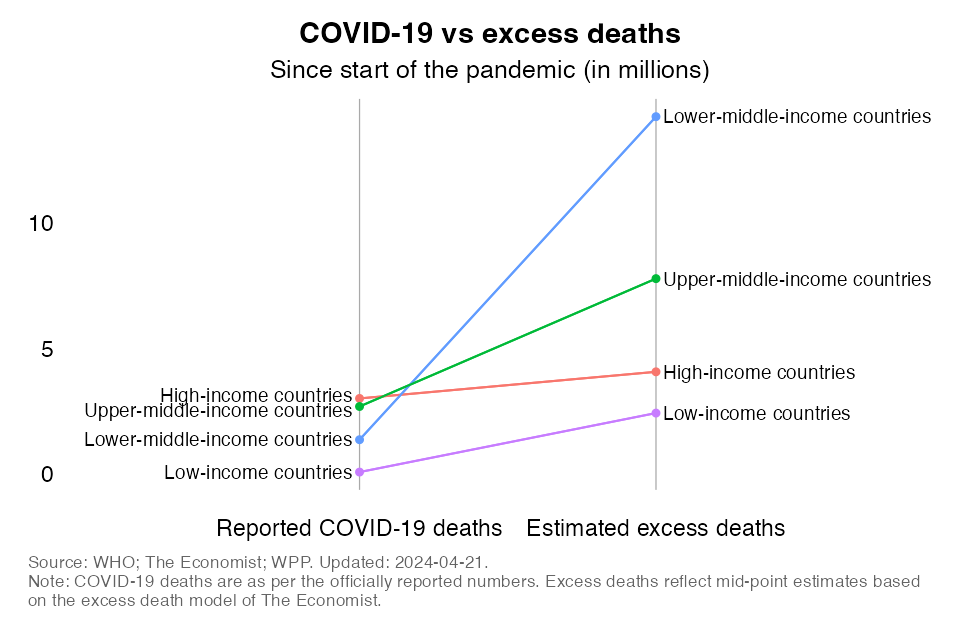
In the charts below, we contrast reported COVID-19 deaths with estimated excess deaths.
First, let’s look at the results by World Bank income group. The left axis in the chart immediately below expresses the absolute mortality toll in millions for each income group; the right axis shows the mid-point excess mortality count. It shows us three things: (1) how similar the numbers on the two axes are for HICs, (2) how the slope of the line dramatically steepens particularly for LMICs and UMICs, and (3) how the lion share of global excess mortality is claimed by middle-income countries (i.e. LMICs and UMICs).
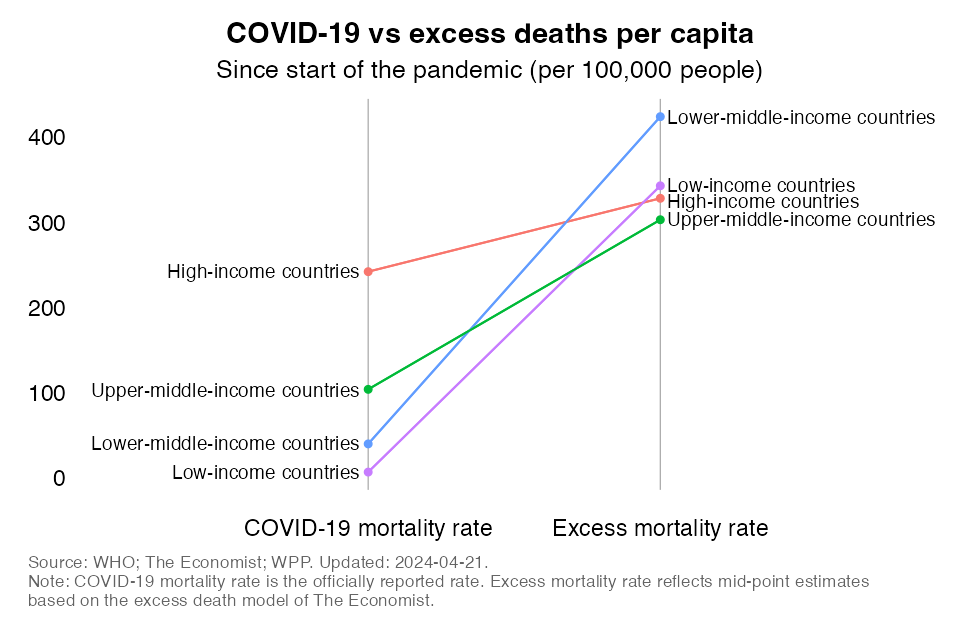
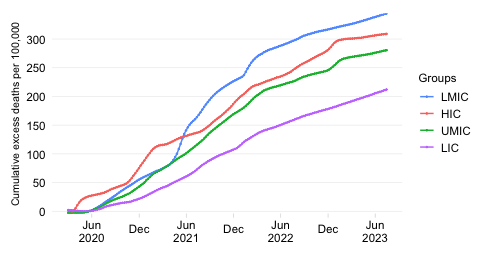
The chart immediately above illustrates why global health has not been subverted. The chart provides a relative view by expressing mortality per 100,000 people. Whereas HICs have the highest reported COVID-19 death rates, LMICs top the ranking for excess mortality rates. Excess death rates in UMIC are similar to those of HICs and those of LICs are a lot higher than what the reported data suggest.
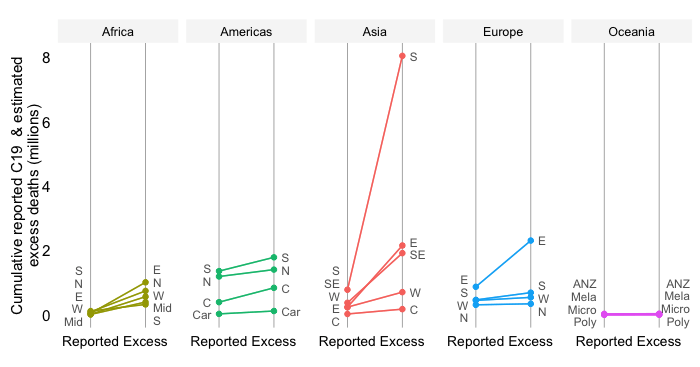
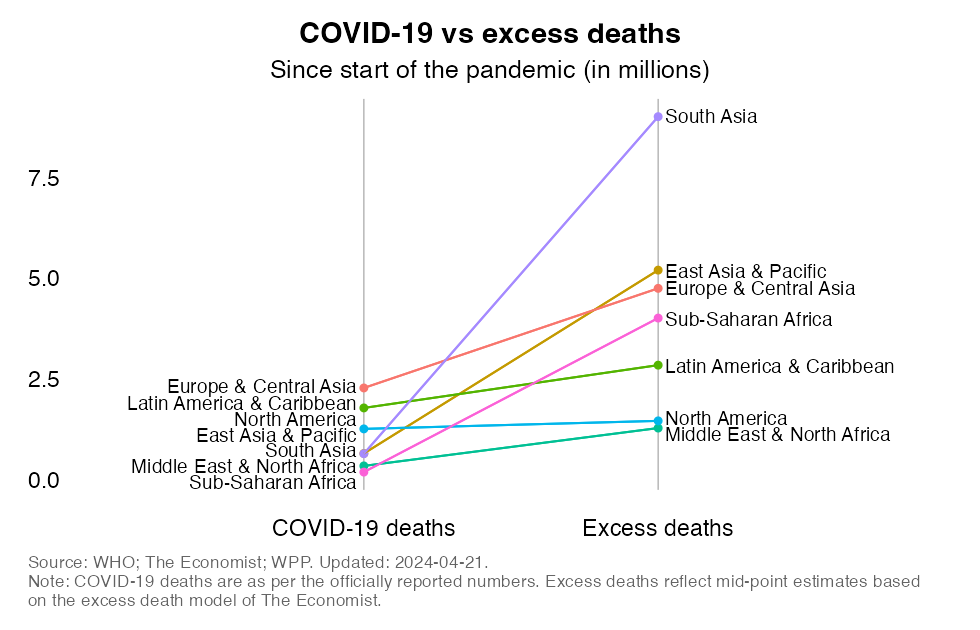
Let us now look at the differences from a geographical point of view and use the World Bank’s regional classification that divides the world into 7 regions.
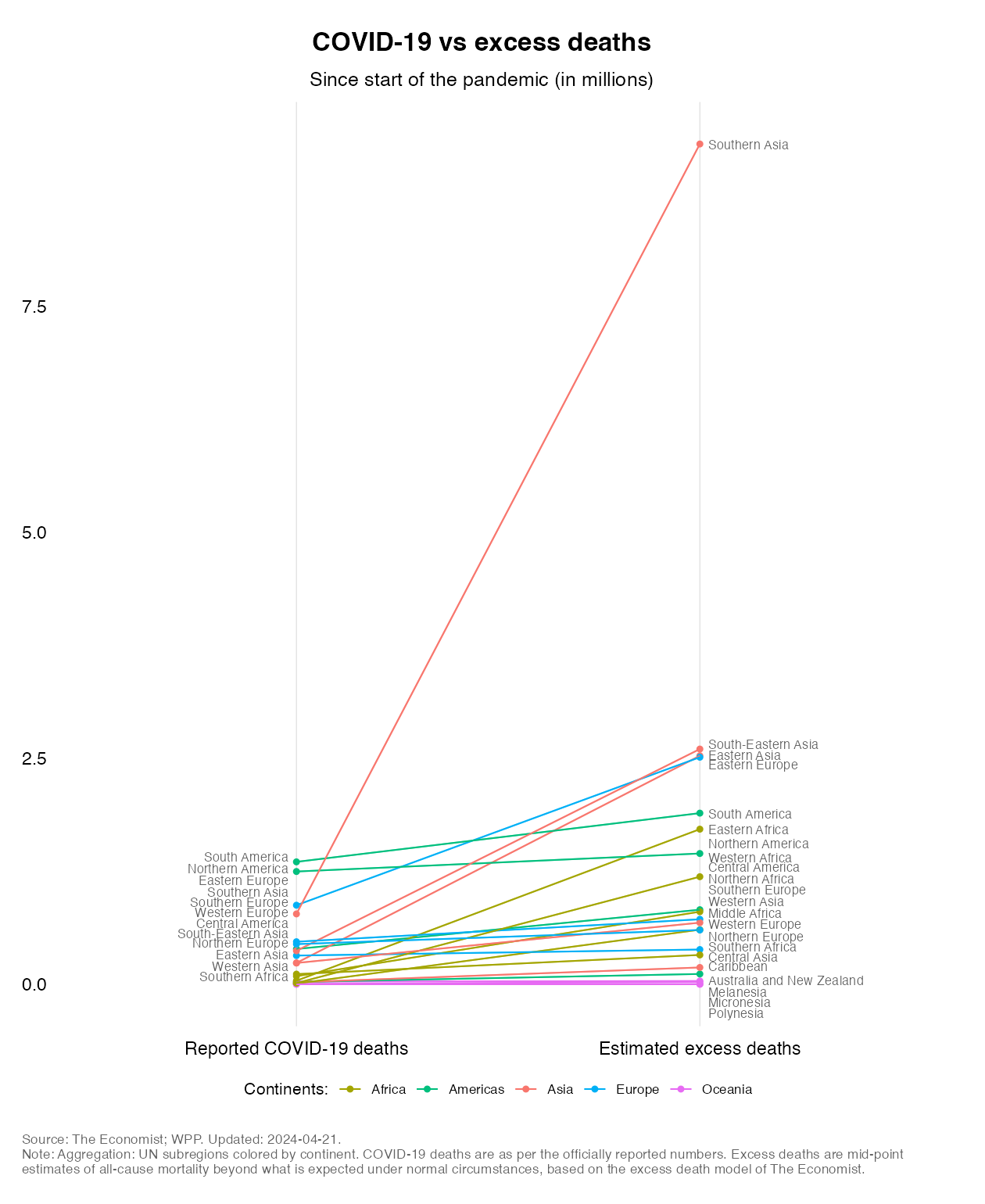
The absolute comparisons in the chart immediately below suggest that South Asia is responsible for most of excess mortality. Second is Europe & Central Asia and third is East Asia & Pacific. (Note that North America might optically look as if it sees a decline, but actually it rises marginally.)
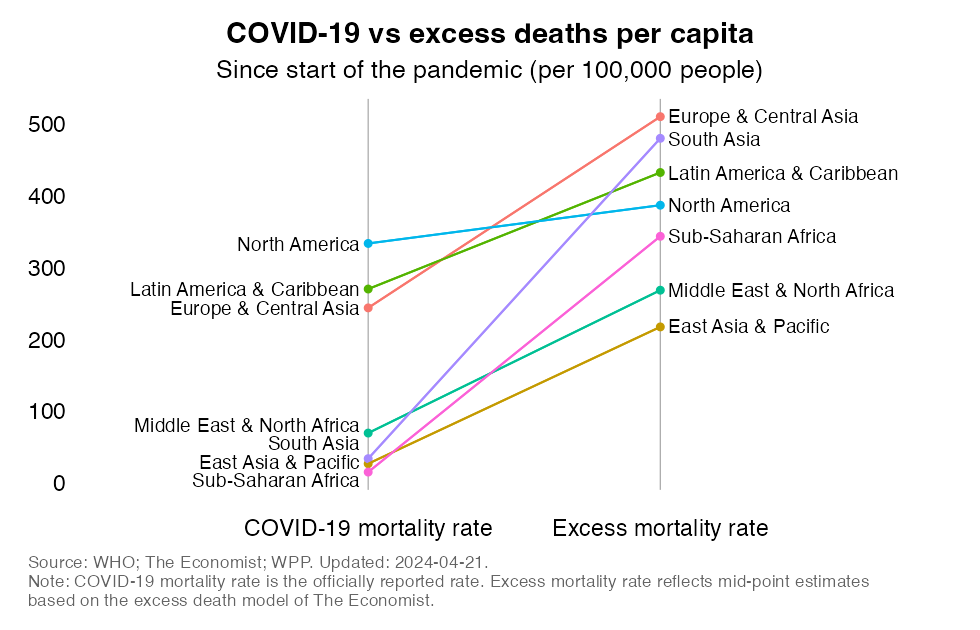
The relative comparisons suggest that Europe & Central Asia have the highest cumulative excess mortality rate. This is closely followed by Latin America & Caribbean, South Asia and North America. Sub-Saharan Africa and East Asia & Pacific are at the bottom. Note also the large differences in slope across the different regions, with South Asia and Europe & Central Asia having the steepest slopes and North America showing the flattest one.
The World Bank’s regional classification is rather aggregate and divides the world into regions that combine geographic areas (for internal reasons) that may exhibit very distinct patterns (e.g. Europe and Central Asia). Let us therefore also look at the subregional classification of the UN, which provides more granular detail.
What pops out even more now in the absolute comparison is the contribution of Southern Asia. This subregion stands out completely and makes all other regions pale in comparison. Of course that is, in large part (though not exclusively), driven by the contribution made by India, which is set to overtake China in 2023 as the country with the largest population in the world.
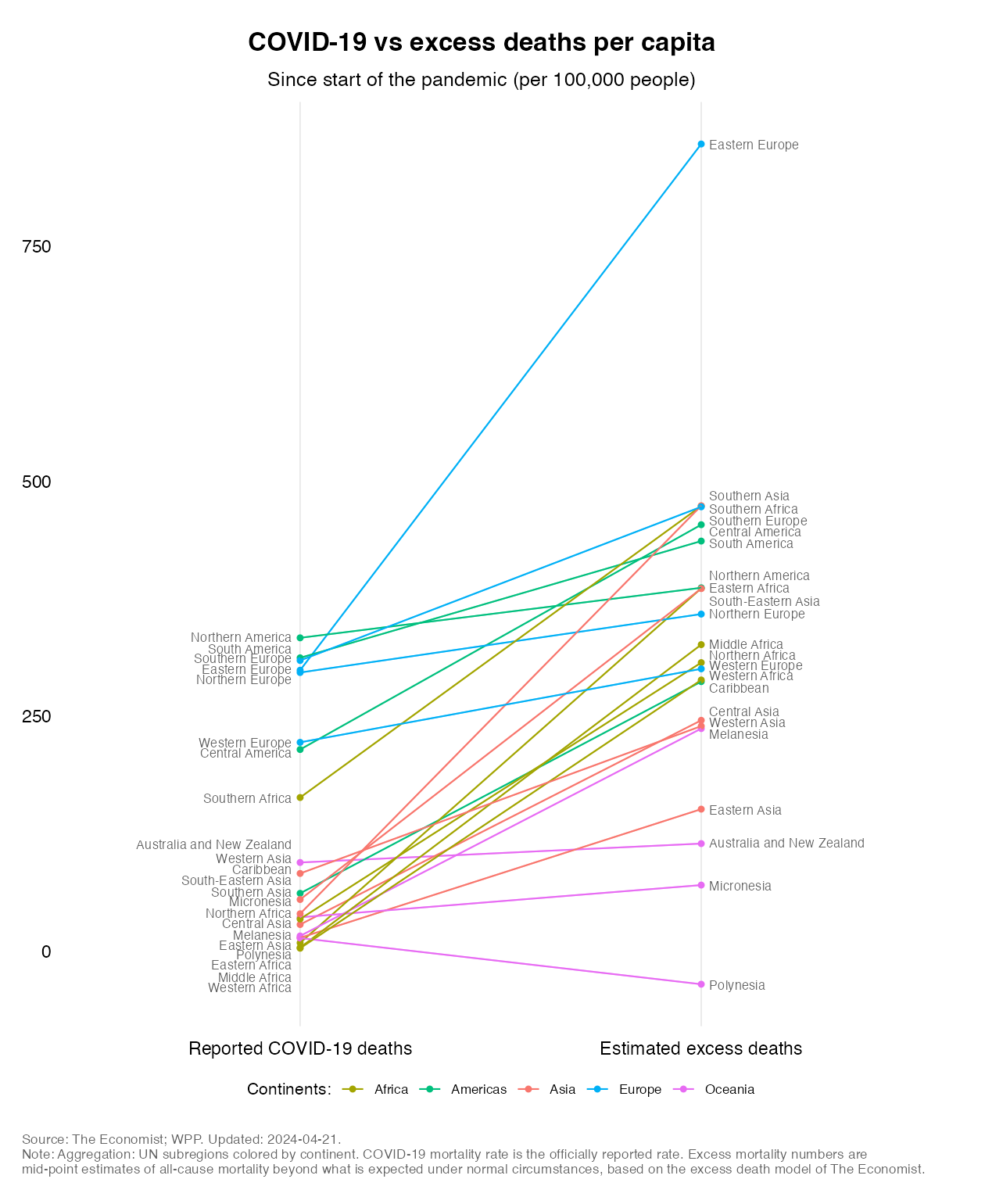
Interestingly, on a per capita basis, it is Eastern Europe that stands out both in terms of slope and level: it has by far the highest excess mortality rate and the discrepancy with the official data is also the greatest in this region. This is for the most part driven by Russia according to the estimates by The Economist. Southern Africa, Central America (which includes Mexico as per the UN’s geo-scheme) and Southern Europe follow closely. The other pattern that is remarkable is that how the lines in some regions are relatively flat, such as in Norther Europe, Western Europe and Australia & New Zealand.
What to make out of all of this? In answering that question let’s return to the perspective of the global mortality distribution by World Bank income classification – as we will argue, the proxy of development afforded by the income classification will matter more than whether or not a country happens to be located in a particular geographical region.
The chart below recaps the result to be explained. It presents the same data that we reviewed before, but this time not as absolute totals or relative rates, but as shares in global totals (the global total for reported COVID fatalities and the global total for estimated excess deaths). We also add the “developing world” group into the income classification, which includes all countries that do not belong to the HIC group and thus consists of the UMICs, LMICs and LICs.
The high-income share in what we think is the true death toll of the pandemic is estimated to be substantially lower than the share in what is reported. Indeed, the HIC share in estimated excess mortality is 16%, whereas the share in officially reported COVID-19 deaths is 42%. These are cumulative numbers as of the latest date available.
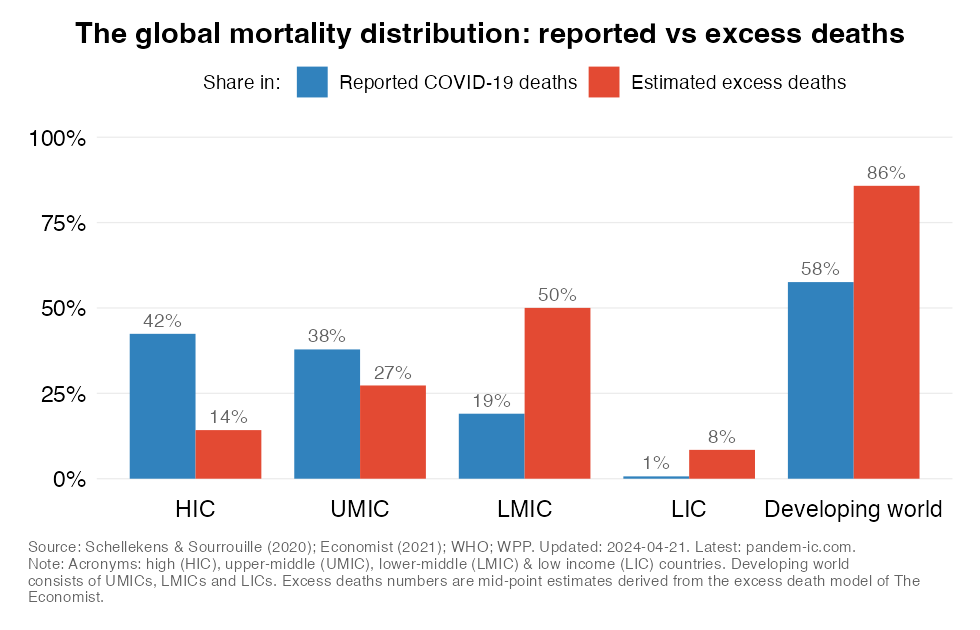
By definition, the patterns observed in the developing world are the mirror image here of what transpired in the HICs, since we’re dealing here with shares in global totals. Thus, the share of the developing world in excess mortality is currently 84%. This is well above its share of 58% in what has been reported so far.
Note however the stark differences within the developing world. The numbers go down for UMICs as we move from reported COVID deaths to estimated excess deaths, but they go up much more considerably for LMICs and LICs. The LMICs stand out with a share in excess mortality that is 2.5x the share in reported mortality. The LIC share in excess mortality is lower, but its discrepancy with reported mortality is the greatest: the difference reflects a factor of 9.1.
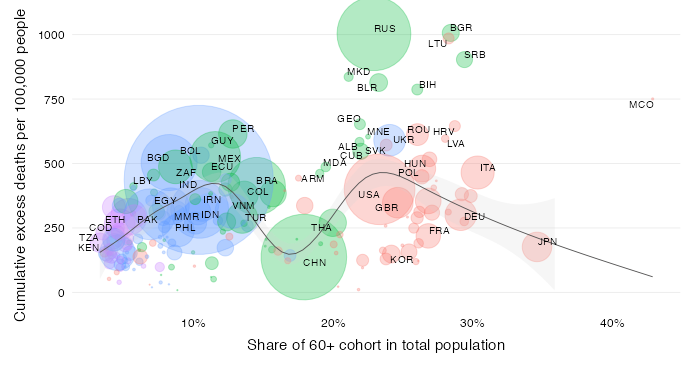
One reason why developing countries contribute so much to the global mortality picture is obviously demography. With demography we refer here to two aspects in particular: population size and population age structure. Developing countries have generally young populations with low elderly shares, but because their overall population is so large we do find their elderly populations are huge in the absolute. So we get the results that while developing countries have younger populations than HIC countries, the population size of the elderly cohorts of developing countries exceeds that of HICs by a significant margin.
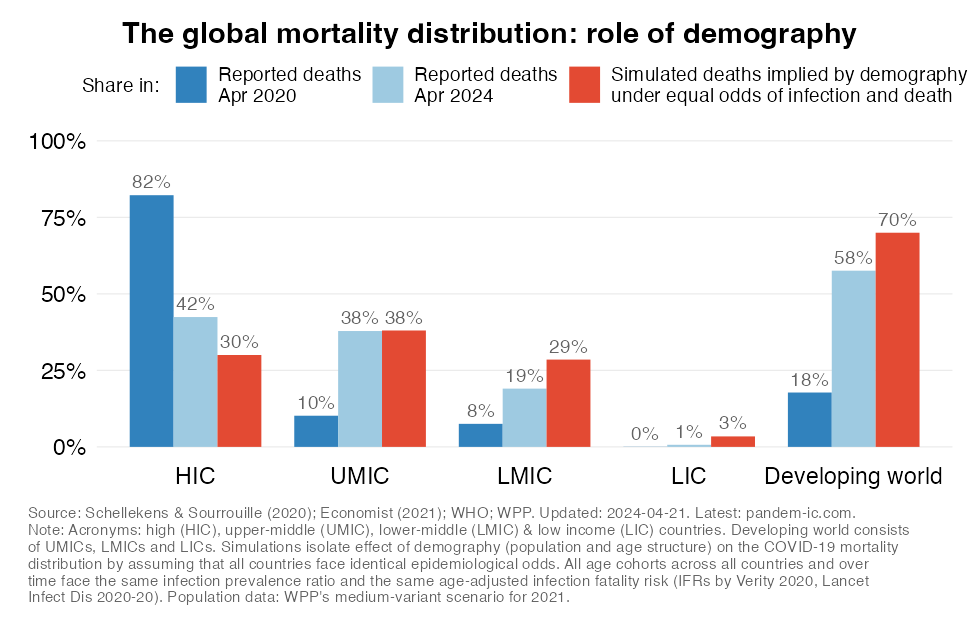
This is why we predicted back in April/May 2020 that the developing country share in the global COVID-19 death toll would rise to at least 70% based on demography alone. Back then the share stood at just 16%. Sadly, this prediction has come true and the increase has more than materialized (see next subsection for the excess mortality perspective). At the time, though, the prospect of such a massive shift of the mortality burden to the developing world seemed unfathomable (as this article in the Guardian discusses).
How did we arrive at the 70% prediction? The simulation isolates the effect of demography, which captures here both population size and age structure. We simulated the hypothetical post-pandemic distribution of the global death toll under the assumption that all countries are equal in the way the pandemic affects them, except for population size and age structure. In other words, we assume that everyone gets infected equally and conditional on their age face the same risk of death given infection.
The simulations capture two opposing effects. First, richer countries are older so they should attract higher mortality rates on account of purely age structure (in other words, their share in global mortality should exceed their share in global population). Second, rich countries are less populous than poorer countries, so while we would expect they have higher mortality rates, their actual share in global mortality should be a lot smaller than the share of poorer countries given the differences in population size.
Let us now combine the previous two insights – that excess death shares exceed reported death shares and that demographically-inspired all-else-equal simulations of the global mortality distribution exceed reported death shares.
The chart below shows in the first bar (in blue) the all-else-equal simulations. Again, asides from demography, all else is kept equal: everyone around the world, in rich and poor countries, face the same epidemiological odds in terms of getting infected and facing death once infected. In other words, infection prevalence rates (IPRs) are constant and identical across countries, age cohorts and over time; age-adjusted infection fatality rates (IFRs) vary across age cohorts but are the same across countries and over time. The second bar (in red) then shows the mortality distribution through the lens of excess death estimates.
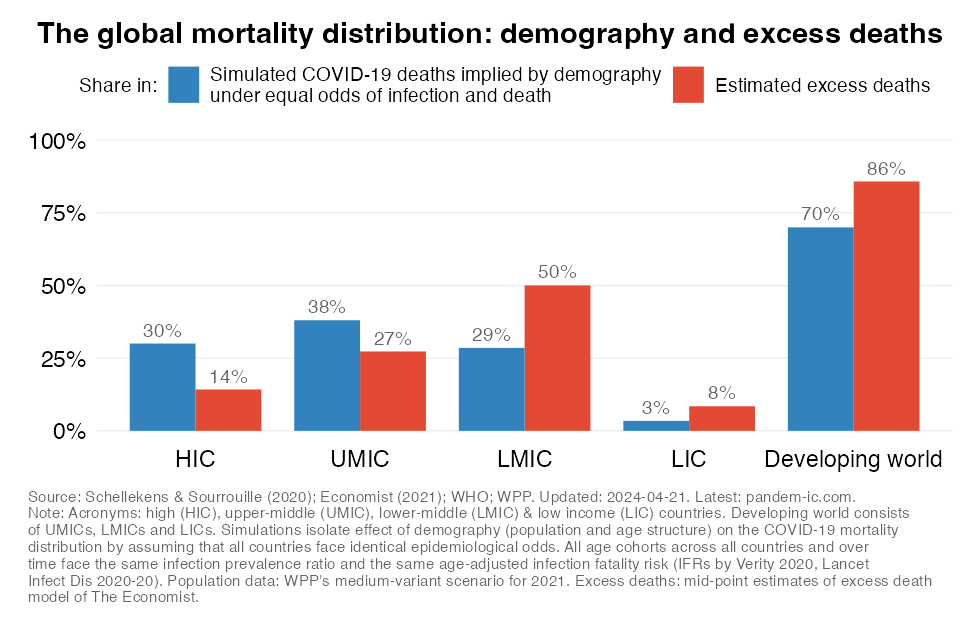
The fact that the excess death share of the developing world is well above the all-else-equal simulations of the mortality toll suggests a combination of two things: that epidemiological odds have been much worse for the developing world (i.e. higher infection prevalence rates and/or higher age-adjusted infection fatality rates) and/or that the non-COVID-19, indirect effects of the pandemic as captured by excess deaths have been more pronounced.
The above conclusion is diametrically opposite to the notion that “COVID-19 has subverted global health” in the sense that we have seen a reversal in the countries traditionally most-affected by a disease pandemic (i.e. HICs instead of lower-income developing countries).
Not only did the absolute death toll (and hence the share in global deaths) catch up with the world’s demographic reality, we are also experiencing far higher death tolls in per capita terms in several countries and regions. These are filtering through the income classification and elevating developing country rates well above those of high-income countries.
We can think of many structural reasons why that would be the case. Infection prevalence has likely been fueled by environmental factors such as urban density as well as poverty and informality, which complicate physical distancing. Over 1 billion people, mostly in developing countries, live in slums. Flattening the curve will therefore be more difficult in many developing countries, meaning that preexisting health capacity constraints will become binding more quickly.
Age-specific infection fatality rates are also likely more elevated than in HICs. Comorbidities are highly prevalent in the developing world. Of the 1.1 billion people with hypertension, two-thirds live in developing countries. Over the last decade, the number of cases and prevalence of diabetes has risen most quickly in the developing world. Also, limited access to quality health care in developing countries would mean that many ailments would be left untreated or undertreated, heightening vulnerability.
Official data on COVID-19 mortality have fooled us more than once. But the reality is that developing countries have been far more severely affected during the pandemic than is commonly thought. They have borne the brunt of the pandemic’s global mortality impact.
In other words, global health has not been subverted: traditional bottlenecks in developing countries have still exerted a disproportionate influence, reducing and offsetting the benefits of any demographic hedges afforded by a younger population.
COVID-19 acts as a heat-seeking missile speeding toward the most vulnerable. That metaphor applies not just to the rich world; the vulnerable in the rest of the world are not more immune. They have actually proven to be easier targets.
Disclaimer: Posts by the Center for Global Development reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. Likewise, views expressed do not necessarily reflect those of the United Nations, the United Nations Development Programme, its programmes/projects or governments. The designations employed do not imply the expression of any opinion whatsoever concerning the legal status of any country, territory or area, or its frontiers or boundaries.